Upload Prescription
Please attach a prescription to proceed
Please enable JavaScript in your browser to complete this form.
Name
*
First
Last
Email
Phone
*
Address
Address Line 1
City
State / Province / Region
Postal Code
Write Your Prescription ( optional )
Upload Prescription
Click or drag a file to this area to upload.
Which Medicine Do You Want ?
Generic Medicines
Branded Medicine
Submit
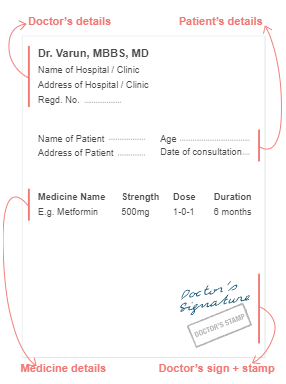
Guide for a valid prescription
Don’t crop out any part of the image
Avoid blurred image
Include details of doctor and patient + clinic visit date
Medicines will be dispensed as per prescription
Supported files type: jpeg , jpg , png , pdf
Maximum allowed file size: 5MB